
Monzón Moreno A1, Merino Bohórquez V2, Villalba Moreno A1
1 Faculativo Especialista de Área. Farmacia de Hospital. Hospital Virgen del Rocío. Sevilla (España)
2 Faculativo Especialista de Área. Farmacia de Hospital. Hospital Virgen Macarena. Sevilla (España)
____
Rev. OFIL 2016, 26;2:103-110
Fecha de recepción: 10/08/2015 – Fecha de aceptación: 25/10/2015
____
SUMMARY
Objective: Evaluate the efficiency of automated dispensing cabinet (ADC) in a ward of internal medicine.
Methods: Cross-sectional study to compare the drug stock, order and organization of the drugs, existence of expired drugs and the drug consumption, in a year, on two wards of internal medicine. One of the wards had an AAD (Omnicell inc.) and the other had a ward stock system. We also performed a calculation of the time needed to pay-off the investment on the ADC.
Results: The drug stock in euros in the ward without ADC was 12,889 euros, while in the ward with ADC was 5,080 euros, a 60.58% lower. On the ward without ADC there were a large amount of deficiencies in the storage of drugs. The total number of individual drugs issued in the ward without ADC over a year was 68,686 units (87,240 euros), in the ward with ADC was 29,884 units (7,490 euros), a 56.49% lower (a difference of 13,750 euros, that is a 15.7% lower in euros). If the cost of the implementation of an ADC in 5 years is 61,000 euros, it could be payed-off in 4.4 years, or 4.6 year assuming a 5% discount rate.
Conclusions: We have demonstrated that ADCs can reduce the drug stock and drug consumption on a ward of internal medicine during a year, compared with another ward with ward stock. The economic savings provided by the ADC can pay-off the investment 4.4 years. The ADC provides also other logistic benefits and in the order and organization of the drugs on the ward.
Key Words: Efficiency [Mesh], hospitalization [Mesh], costs and cost analysis [Mesh], electrical equipment and upplies [Mesh].
____
Correspondencia:
Antonio Monzón Moreno
Avda. Concejal Alberto Jimenez Becerril, 26
(bloque 2, escalera 2, 3º-3)
41009 Sevilla
Correo electrónico: amonzonm2@gmail.com
____
Introduction
Automated dispensing cabinets (ADC) are a computerized drug storage device. ADCs allow drugs to be stored and dispensed near the point of care while the control and track the drug distribution. Hospital pharmacies have traditionally provided drugs to the wards through the ward-stock system. The ADCs are designed to replace non-automated ward stock storage and have facilitated the transition to alternative delivery models and more decentralized medication distribution systems. ADCs can improve patient safety and the accountability of the inventory, reduce costs and lead to increased nursing and patient satisfaction. Because automated dispensing cabinets track user access and dispensed medications, their use can improve control over medication inventory. The real-time inventory reports generated by many cabinets can simplify the filling process and help pharmacy track expired drugs. Furthermore, by restricting individual drugs –such as high-risk medications and controlled substances– to unique drawers within the cabinet, overall inventory management, patient safety, and medication security can be improved. Automated dispensing cabinets allow the pharmacy department to profile physician orders before they are dispensed.
Automated cabinets can also enable providers to record medication charges upon dispensing, reducing the billing paperwork pharmacy is responsible for. In addition, nurses can note returned medications using the cabinets’ computers, enabling direct credits to patients’ accounts. Since automated cabinets can be located on the nursing unit floor, nursing have speedier access to a patient’s medications. Decreased wait time for medication can lead to less frustration for nursing staff and prevent conflict between the pharmacy and nursing staff. Also, shorter waiting time ensures improved patient comfort and care.
The most important thing a hospital pharmacy should enforce is the patient safety. Wrong drug and wrong dose errors are the most common errors associated with ADC use. Look-alike drug names and drug packages are common variables that lead to selection errors.
Automated dispensing cabinets (ADCs) are quickly becoming the solution of choice for point-of-care medication administration. By 2007, more than 80% of hospitals of USA had implemented them, according to the Institute for Safe Medication Practices (ISMP). Their benefits include improved nurse access to medications, more efficient medication billing and inventory management, greater medication security, and potential reductions in medication errors.
In our study we are going to evaluate the efficiency of an ADC in a ward of internal medicine compared with a ward of very similar characteristic but with a ward stock system.
Material and methods
We preformed a cross-sectional study to compare the drug stock, order and organization of the drugs, existence of expired drugs and the drug consumption, in a year, on two wards of internal medicine. One of the wards had an ADC (Omnicell inc.) and the other ward had a ward stock system. We also performed a calculation of the time needed to pay-off the investment on the ADC.
The study was made in four parts:
- Accounting of drug stock in euros, in both wards: On February, 20th, 2011 a cross-sectional accounting of the drug stock on both wards was made.
- Order and organization of drugs and existence of expired drugs, in both wards: On February 20th, 2011, at the same time of the accounting, the order and organization in which the drugs were in each ward, was examined (correct identification, correct conservation, proper location, existence of expired drugs, etc.). Since this part was a qualitative study, no formal coding system was used, only YES or NO variables were used to evaluate every parameter.
- Drug consumption in a year, in both wards: The drug consumption was evaluated from February 20th, 2011, till February 20th, 2012, in both wards. We calculated the number of individual drugs issued (number of tablets, capsules, vial, etc), the cost of the drugs consumed in each ward during a year. We also calculated the cost savings in drugs resulting from the implementation of the ADC during a year. On the ward without ADC, the data of drug consumption was obtained from the pharmacy department inventory management program. On the ward with ADC, data of the drug consumption was obtained from the computer system of the ADC.
- Calculation of the time needed to pay-off the investment for the implementation of the automated dispensing cabinet: We calculated the cost of implementing the ADC on the ward and the time necessary to pay it off by the cost savings in drugs.
The study was carried out at Hospital Virgen Macarena in the city of Seville (Spain), this a public and tertiary hospital that belongs to the Andalusian Health Service (Andaluz de Salud), comparing two internal medicine wards on the 8th floor, the ward 8th-A had an ADC (model Color Touch, Omnicell inc.) and the ward 8th-B had a ward stock system.
The two wards served the same type of patients (internal medicine patients) and the physicians working on both wards were the same. The patients were randomly assigned to each ward based only in the availability of beds. This was because both wards belonged to the same department and to the same physicians, they were only fiscally separated by a door on the same floor. This was the prefect scenario to compare two groups were the only difference was the medicine distribution. Ward 8th -A had 29 beds and ward 8th-B had 27. The ADC was configured in Stocked Medications Level, we did not have implemented the Profile Medications Level or the Scheduled Medication Level by that time. The calculated drug stock and the drug consumption data were corrected to compensate for the difference in the number of beds between the two wards.
During the previous 3 years both wards had the same evolution on costs an 8% increase in costs every year.
The study variables were of two types:
Quantitative variables: drug stock and drug consumption in a year.
Qualitative variables: deficiencies on organization (that included: order and organization of the drugs, workflow processes and existence of expired drugs).
The drug stock on each ward was calculated using the costs of medicines that were paid by the hospital during the year of the study (2012-2013). To calculate the time needed to pay-off the investment, we present it in two ways, one without a discount rate and second with a 5% discount rate.
The automated dispensing cabinets (ADCs) store and dispense the medication on the ward. The ADCs are electronically controlled and are integrated into the network of the hospital. The ADCs provides advantages, such as the automatic generation of orders for replenishment, medication control and safety in the prevention of medication errors. The ADCs can be configured at three different levels1,2:
A.- Stocked Medications Level: This is the basic level, once the nurse accesses the cabinet, the cabinet displays the list of patients of the ward on the screen. After the nurse selects a patient, the cabinet displays the list of drugs stocked in the cabinet. The nurse can then remove the drugs for the patient. All of this is done without the need of a computerized prescription. Access can be restricted according to the user and the type of medication.
B.- Profile Medications Level: To issue a drug the automated dispensing cabinet (ADC) needs a computerized physician order. This requires the existence of an interface from an e-prescribing system that sends then computerized physician order to the ADC. Once the nurse has selected the patient from the screen, the cabinet displays the prescribed drugs for that patient. With this stage, the nurse can only remove drugs that are prescribed. The nurse can also have access to drugs that are not prescribed through another screen, but in this case a message of “drug not prescribed” will appear. In some cases and based on hospital processes, select medications are available as an “override” depending on the user or type of medication.
C.- Scheduled Medications Level: To remove a drug the ADC, the ADC can provide a filtered list of the physician orders based on the time frame that they are to be removed and administered to the patient. This is an advanced version of the profiling seen before. Once the nurse has selected the patient from the screen, the cabinet displays the list of prescribed drugs for that patient in that time frame. Once the drug is removed, it disappears from the list of drugs to be administered in that time frame and if the nurse returns the drug, it will reappear in the list based on time parameters determined by the hospital.
With each of these levels, there is increasing security and safety that is provided for ADC’s.
In this study we compared the level of stocked drugs, the overall organization and workflow process associated with drugs, the existence of expired drugs and the consumption of the drugs in a year, in two wards of internal medicine at a tertiary hospital. We also made a calculation of the time necessary to pay-off the cost of the implementation of the ADC.
The study was made in four parts:
- Accounting of drug stock in euros, in both wards: On February, 20th, 2011 a cross-sectional accounting of the drug stock on both wards was made.
- Order and organization of drugs and existence of expired drugs, in both wards: On February 20th, 2011, at the same time of the accounting, the order and organization in which the drugs were in each ward, was examined (correct identification, correct conservation, proper location, existence of expired drugs, etc.).
- Drug consumption in a year, in both wards: The drug consumption was evaluated from February 20th, 2011, till February 20th, 2012, in both wards. We calculated the number of individual drugs issued (number of tablets, capsules, vial, etc), the cost of the drugs consumed in each ward during a year. We also calculated the cost savings in drugs resulting from the implementation of the ADC during a year. On the ward without ADC, the data of drug consumption was obtained from the pharmacy department inventory management program. On the ward with ADC, data of the drug consumption was obtained from the computer system of the ADC.
- Calculation of the time needed to pay-off the investment for the implementation of the automated dispensing cabinet: We calculated the cost of implementing the ADC on the ward and the time necessary to pay it off by the cost savings in drugs.
A narrative review was carried out using PUBMED, grey literature, including the web page of the Spanish Society of Hospital Pharmacy magazine, for studies published from 1992 to 2012.
Results
The results have been divided into four parts according to the materials and methods:
- Accounting of the drug stock in euros, in both wards:
The accounting of the stock of drugs on the ward without ADC was more complex since the work had to be done manually and the drugs were distributed on to different shelves. The accounting of the stock of drugs on the ward with ADC was obtained easily through the computer system of the ADC and all of the drugs were located in the same cabinet.
The drug stock in euros in the ward without ADC was 12,889 euros, while the drug stock in euros in the ward with ADC was 5,080 euros. Hence, the drug stock in the ward without ADC in euros is more than double than the ward with ADC, exactly, the drug stock in euros in the ward with ADC was a 60.58% lower.
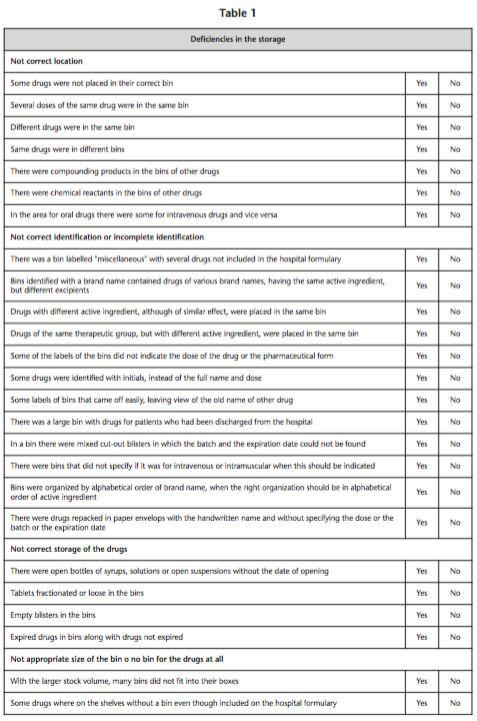
- Overall organization, workflow processes and existence of expired drugs, in both wards:
After reviewing the order and organization of the drugs and the existence expired drugs, on the ward with ADC and the ward without ADC, we found there was a large amount of deficiencies in the storage of drugs in the ward with out ADC (Table 1).
- Drug consumption in a year, in both wards:
The data of the number of issued drugs and the drug consumption in the ward without ADC was obtained from the pharmacy department inventory management program. While on the ward with ADC, was obtained from the computer system of the ADC.
The number of individual drugs (tablets, capsules, vials, etc) issued in the ward without ADC over a year was in total 68,686 units, while in the ward with ADC over a year was 29,884 units. Hence, the total number of individual drugs issued on the ward without ADC was more than double than the ward with ADC. Exactly, the total number of drugs issued in ward with ADC was a 56.49% lower.
The cost of the drugs consumed (total drug consumption) on the ward without ADC was 87,240 euros over a year, while the cost of the drugs consumed (total drug consumption) on the ward with ADC was 73,490 euros over a year, indicating that there was a reduction in the drugs consumed during a year of 13,750 euros, what means a reduction of a 15.7% in drug consumption (Table 2).
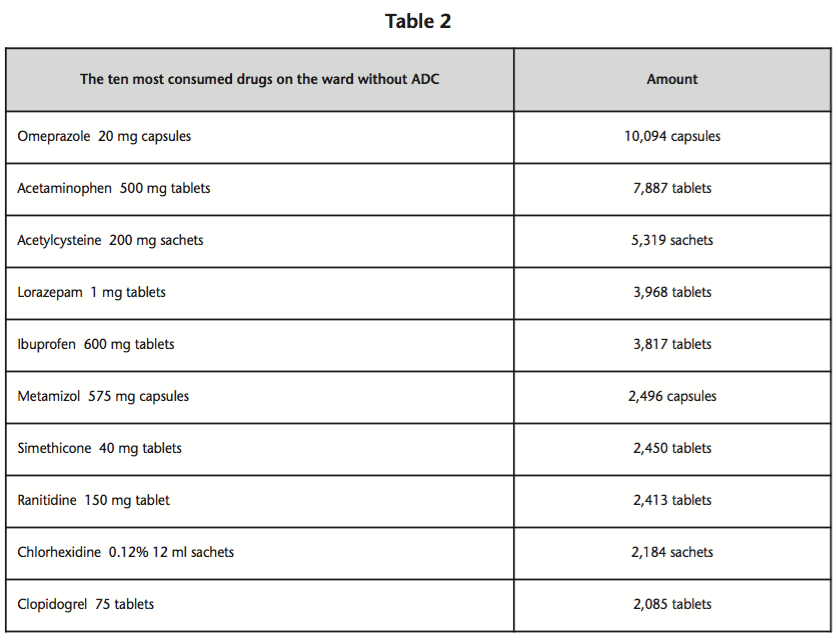
The drug consumption was lower in the ward with ADC, than in the ward without ADC. The majority of the ten most consumed drugs were drugs of popular use, for mild diseases, OTC (over the counter) or those drugs which not require a prescription, except for the case of lorazepam and clopidogrel that require prescription.
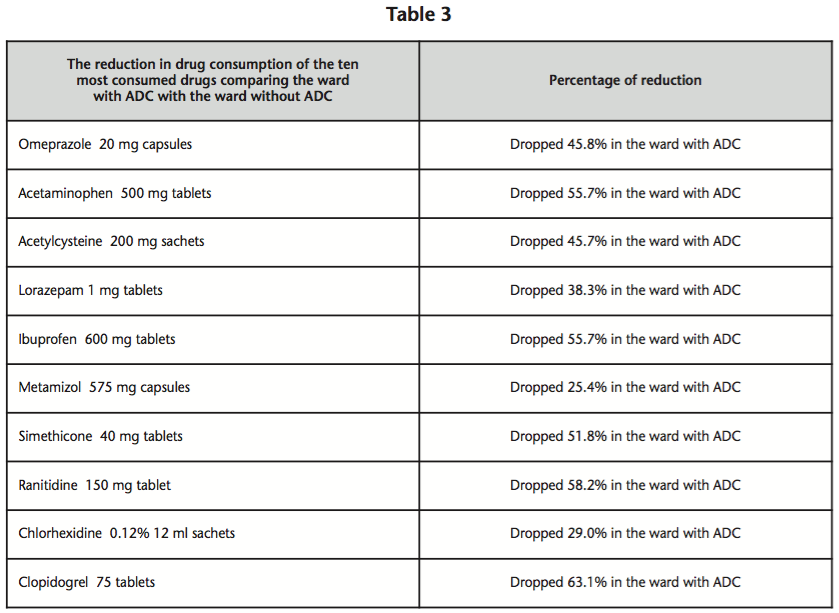
The reduction in drug consumption of the ten most consumed drugs comparing the ward with ADC with the ward without ADC shows in table 3.
The consumption of injectable drugs was not affected by the implementation an ADC compared with the ward without ADC, the main difference was observed in the metamizol 2 gram vials, who presented a higher consumption in the ward with ADC than on the ward without ADC. The reason for this is probably because injectable drugs are not easy to use out of the hospital facility.
Other benefits provided by the implementation of an ADC was that the need for replenishment of the ward was reduced to only 3 times per week (in working days), compared with the ward without ADC, which required daily replenishments (in working days). Also the ward without ADC had a high number orders for individual drugs, while in the ward with ADC there was no need for these orders.
- Calculation of the time needed to pay-off the investment of the implementation for the automated dispensing cabinet:
The cost of our ADC was 45,000 euros, to this cost we added the cost of the maintenance carried out by the installation company, which included periodic reviews, replacement of hardware, replacement of drawers or shelves, computer maintenance (attention to computer incidents, integration of interfaces with the pharmacy programs) and the maintenance of the computer server that controls the ADC and its remote access, with a cost of about 2,000 euros per year for the maintenance of the ADC and 2,000 euros for the maintenance of the server. The cost of the maintenance the first year was free.
The cost of deployment and use of the ADC during the first year was 45,000 euros, the second year we estimate it would increased by 4,000 euros for the maintenance (total: 49,000 euros), the third year we estimate it would be increased by another 4,000 euros (total: 53,000 euros), the fourth year we estimate it would be increased by another 4,000 euros (total: 57,000 euros) and the fifth year we estimate it would be increased by another 4,000 euros (total: 61,000 euros).
In the evaluation of the consumption of drugs we concluded that the ward with ADC achieved a reduction in drug consumption of 13,750 euros in the first year, we can assume that this reduction in consumption would be equal the following years.
If we divide the cost of the ADC during 5 years (61,000 euros, which is the cost of the ADC plus the maintenance) by the savings achieved by ADC per year (13,750 euros), it results in 4.4 years. This is the time we need to pay-off the investment of implementing this technology.
The costs can be calculated using the discount rate (also noun as bank rate). The discount rate refers to the interest rate used in discounted cash flow (DCF) analysis to determine the present value of future cash flows. Assuming a 5% discount rate, then if the cost of the ADC was 61,000 euros (45,000 euros from the cabinet plus 16,000 euros from the maintenance), the final cost increasing a 5% discount rate would be: 64,050 euros.
Again, if we divide the cost of the ADC during 5 years with the discount rate (64,050 euros, which is the cost of the ADC plus the maintenance) by the savings achieved by ADC per year (13,750 euros), it results in 4.6 years. This is the time we need to pay-off the investment of implementing this technology.
Discussion
The pharmacy departments in hospitals are under continuous development, one of the most current development lines is the automation of the dispensing process. There are publications about the benefits of the ADC in the ICU and emergency room areas. There are some other studies on the outpatient setting where the ADC have also demonstrated a benefit/cost ratio favourable. There is a need for publications on the implementation of ADC in areas of hospitalization in order to evaluate the effect of this technology in that area.
Poveda et al.3 evaluated the monetary impact when traditional drug floor stocks were replaced by automated drug dispensing systems (ADDS) in the intensive care unit and in the emergency room. They concluded that traditional floor stocks by ADDS in the intensive care unit and the emergency room produces a positive benefit/cost ratio (1.95).
Perez-Ruixo et al.4 evaluated the implementation of ADC in the emergency department of a tertiary hospital and concluded that the implementation of an automated dispensing system reduced the cost of the medication used. They found out that the cost of the medication used during the first three months of the year 2000 was a 13.64% lower that the cost in the same period during the previous year. This economical result is very similar to the one of our study, a reduction of a 15.7% in drug consumption, in our study was in an internal medicine ward.
Perez-Ruixo et al.5 published a study that does not evaluate the reduction in costs, but present some advantages of the ADC in the intensive care unit. They demonstrated that during the first semester of 1996, a total of 442 drugs were consumed with a cost of 36 million pesetas. This included 92 drugs that accounted for 42% of the overall medication costs. The system showed a coverage of medical prescription close to 80% and after the training program, its use increased from 56.6% to 78.8%, and errors in dispensing medicines decreased from 18% to 5.7%. Concluding that the systems allow the pharmacist to increase his/her knowledge on the general and individualized use of medicines in the intensive care unit, to participate in therapeutic interchange activities, and to be involved in the individual pharmacotherapy of patients.
Zafra-Fernández et al.6 evaluated in economic terms, the effect of replacing traditional kits for the implementation of automated dispensing of medications in the Intensive Care Unit. Analyze the degree of acceptance of such change on the part of users. For the economic analysis they considered tangible direct and indirect costs resulting from the implementation: initial capital investment, cost of staff involved, the political cost of drug consumption. All these aspects were evaluated before and after implantation. The degree of user satisfaction was assessed using a standardized questionnaire. They concluded that the expenditure incurred on the initial investment could be quickly offset by the cost mainly referred to the politics of consumption of drugs, with a reduction of 24% over the previous delivery system. The cost in personal chapter was also reduced by 11%, and the cost per stay and cost / income fell by 26% and 30% respectively over the previous system. The evaluation questionnaire revealed that users were satisfied with the implementation and 84% of nurses would recommend it to other units. In this study they used an ADC from Omnicell similar to the one we used in our study, they reached a reduction of 24% in drug consumption, while we reached a reduction of a 15.7% in drug consumption, in our study was in an internal medicine ward.
Jorgenson et al.7 evaluated the implementation and analysis of an automated system for the distribution of medications and supplies in an ambulatory clinic setting. Distribution, charging and control of medications and supplies provided to ambulatory clinics is an issue that presents numerous problems for hospital pharmacy departments. A combined automated unit to handle both supplies and medications was studied as an alternative to traditional manual systems. Jorgenson et al found problems with their manual system. A comparative of revenue, medication and supply cost before and after automation was presented. A 7% increase in revenue, decreases in supply cost and improved medication expense documentation were noted with the automated system. As we have found in our study, the ward stock system presents numerous problems, also, their economical results are very similar to the one of our study, a reduction of a 15.7% in drug consumption, in our study was in an internal medicine ward.
Alvarez-Rubio et al.8 evaluated the effect of an automated dispensing system in the emergency department of a tertiary hospital. They concluded that the main benefit of this system was the information it provides on drug use. The implementation of the automated dispensing system increased the workload in the pharmacy department. The drug consumption in the emergency department was reduced by 12% in 2001. In addition, the number of applications (orders) for drugs not included within the hospital formulary decreased. This economical result is very similar to the one of our study, a reduction of a 15.7% in drug consumption, in our study was in an internal medicine ward.
Tsao et al.9 conducted a literature search in MEDLINE, Embase, and all evidence-based medicine databases for the years 1992 to 2012 to identify English-language articles reporting on the use of ADC in hospital wards. Of 175 studies initially identified, 8 were retained for evidence synthesis. It appears that ADC were effective in reducing medication storage errors and the time that nurses spent taking inventory of narcotics and controlled substances. There was no definitive evidence that using ADC increased the time that nurses or pharmacists spent with patients, reduced medication errors resulting in patient harm, or reduced costs in Canadian hospitals. However, pharmacy technicians spent more time stocking the machines. The concluded that the ADC have limited potential to decrease medication errors and increase efficiencies, but their impact is highly institution-specific, and use of this technology requires proper integration into an institution’s medication distribution process.
Limitations of our study should be considered when analyzing the results. Although the research of our study has reached its aims, there were some unavoidable limitations. First because of the time limit, this study was conducted only in a small size unit (two wards of internal medicine), therefore, to generalize the results for larger groups, the study should have involved more hospital wards and at different medical units. Its single-center nature limits its external validity. Further multi-center studies or single-center studies are necessary to verify the reproducibility of our results.
Another limitation of the study was that the measurements were made without blinding of the researcher, which has the potential for bias. Another limitation is that even though the patients were assigned to any of the wards without considering the presence of an ADC, we have not balanced or evaluated the type of patient, age or pathology in the two wards, there could be a bias in the groups.
Conclusions
The ADCs can reduce the drug stock and the drug consumption. The economic savings provided by the ADC can pay-off the investment made by the hospital in 4.4 years. The ADC provides also other logistic benefits and in the order and organization of the drugs on the ward.
Competing interests: The authors declare no conflicts of interest.
BIBLIOGRAPHY
- Monzon Moreno A, Guerrero Aznar MD. Guía básica para la instalación de armarios automáticos de dispensación. OFIL 2010;20(1-2):18-30.
- Monzon Moreno A. Nuevas tecnologías para la seguridad del paciente en farmacia hospitalaria. OFIL 2011; 21(1):32-9.
- Poveda Andrés JL, García Gómez C, Hernández San Salvador M, Valladolid Walsh A. Análisis coste-beneficio de la implantación de los sistemas automáticos de dispensación de medicamentos en las Unidades de Críticos y Urgencias. Farm Hosp. 2003;27(1):4-11.
- Perez-Ruixo JJ, Martínez G, Quintana V et al. Impacto farmacoeconómico de la implantación de un sistema de botiquín automatizado en la unidad de urgencias de un hospital general universitario. Farm Hosp. 2000; 24(6):390-7.
- Perez-Ruixo JJ, Pastor E, Juan J, Jiménez NV. Análisis de un sistema automatizado de dispensación individualizada de medicamentos en una unidad de cuidados intensivos. Farm Hosp. 1998;22:81-8.
- Zafra Fernández, JL, Isla Tejera B, Del Prado Llergo JR. An automatic dispensing system medications effect in pharmaceutical expenditure and satisfaction user level. Enfermeria Global 2012:11(25):250-61.
- Jorgenson JA, Leiker T, Herzog C. Combined medication and supply automated delivery system in an ambulatory setting. Hosp Pharm. 2002;37(8):828-32.
- Alvarez Rubio JA, Martín Conde A, Alberdi Lens I. Evaluación de un sistema de dispensación en el Servicio de Urgencias de un hospital de tercer nivel. Farm Hosp. 2002;27(2):72-77.
- Tsao NV, Clifford L, Babich M, Shah K and Bansback NJ. Decentralized automated dispensing devices: systematic review of clinical and economic impacts in hospitals. 2014. CJHP (67)2:138-144.
____
Download PDF: Evaluation of the efficiency of an automated dispensing cabinet (ADC) in a ward of internal medicine