
Fecha de recepción: 15/06/2017 – Fecha de aceptación: 08/09/2017
Stamboulian D1, Soler L1, Copertari P1, Cordero AP1, Vázquez H1, Valanzasca P1, Monsanto H2, Grabenstein JD3, Johnson KD4
1 Fighting Infectious Diseases in Emerging Countries (FIDEC). Miami, FL (USA)
2 Merck Sharp & Dohme. Latin America Health Outcomes Research. Carolina (Puerto Rico)
3 Merck & Co., Inc., Vaccines. North Wales, PA (USA)
4 Merck & Co., Inc., Center for Observational and Real-World Evidence. Vaccines. Kenilworth, NJ (USA)
____
Correspondencia:
Daniel Stamboulian
2050 Coral Way suite 407
Miami, Florida 33145 (USA)
Correo electrónico: dstamb@stamboulian.com.ar
____
Resumen
Introducción y objetivos: En América Latina, la carga de enfermedades prevenibles por vacunas en adultos continúa siendo elevada y se requieren estrategias de salud pública efectivas para mejorar las tasas de inmunización. No está claro si la ley permite a los farmacéuticos vacunar. Las regulaciones que rigen sobre los farmacéuticos como vacunadores varían a través del mundo. Con este estudio, buscamos comprender las políticas y prácticas en torno a la vacunación en la farmacia de la región.
Métodos: Se realizó una encuesta para comprender las políticas y prácticas relacionadas con la vacunación en la farmacia en Argentina, Brasil, Chile, Colombia, México y Venezuela. Se seleccionaron entre dos y seis expertos de cada uno de los países mediante muestreo de conveniencia basado en registros obtenidos de confederaciones, sociedades, academias o consejos nacionales de farmacias, universidades e instituciones de salud pública de cada país, así como organizaciones internacionales como la OPS, el FIP y la OMS.
Resultados claves: Los resultados, basados en las respuestas de los expertos, mostraron que las regulaciones y las prácticas en la farmacia son diversas. En Argentina y México la ley que regula la vacunación en farmacias es clara. Por el contrario, en Brasil, Chile y Colombia, la variabilidad en las respuestas pone de manifiesto que no existe un entendimiento común de las leyes que gobiernan.
Conclusiones: Se deben intensificar los esfuerzos para comprender plenamente las políticas de vacunación en América Latina e implementar políticas habilitadoras en países donde los farmacéuticos no vacunan.
Palabras clave: Instalaciones de atención médica, farmacéuticos, servicios farmacéuticos, servicios de salud preventiva, inmunización.
____
Artículo completo en inglés:
Policies and practices on pharmacy-delivered vaccination: a survey study conducted in six Latin American countries
SUMMARY
Introduction and objectives: In Latin America, the burden of vaccine preventable diseases in adults is still high and public health strategies to improve immunization rates are needed. It is unclear if pharmacists can vaccinate. Regulations for pharmacist to vaccinate vary across the globe. With this study, we aimed to understand the policies and practices around pharmacy-delivered vaccination in this region.
Methods: A survey was conducted to understand the policies and practices around pharmacy-delivered vaccination in Argentina, Brazil, Chile, Colombia, Mexico and Venezuela. Two to six experts of each of the countries were selected by convenience sampling based on registries obtained from national pharmacy confederations, societies, academies or councils, universities and public health institutions from each country as well as international organizations such as PAHO, FIP and WHO.
Key results: Results showed regulations and pharmacy practices are diverse based on the experts’ responses. In Argentina and Mexico the law that regulates vaccination in pharmacies is clear. In contrast, in Brazil, Chile and Colombia, the variability in responses highlights that there is not a common understanding of the governing laws.
Conclusions: Increased efforts should be taken to fully understand policies around vaccination in Latin America and how enabling policies can be implemented in countries where pharmacists do not vaccinate.
Key Words: Health care facilities, pharmacists, pharmaceutical services, preventive health services, immunization.
____
INTRODUCTION
Worldwide, immunization practices prevent between 2 and 3 million deaths every year, and they are one of the most successful and cost-effective health interventions to prevent illnesses, disability, sequelae, hospitalizations and deaths caused by vaccine-preventable diseases such as influenza, pneumonia, and whooping cough1. Pharmacists have demonstrated a critical role in vaccine delivery in several countries2-5.
Despite the availability of effective vaccines, adult vaccination rates remain low. Vaccination in adults is not a common practice in medical care and many physicians do not inform their patients about the vaccines they need. Members of the community are too often unaware of which vaccines they may need to receive. Vaccine-preventable diseases are still prevalent in adults, causing great economic impact, and results in increased medical visits, hospitalizations and premature deaths that could be avoided6. It is important to identify alternative approaches to vaccinating adults, especially the role of pharmacists as vaccinators7-11.
Nowadays, it is necessary to reassess the role of pharmacists in the primary health care system, to promote and safeguard the proper use of medications, to identify signs of need for medical consultation, and to raise awareness of the importance of vaccination and disease prevention12. Various papers emerged in 2011 as joint Guidelines of the International Pharmaceutical Federation (FIP) and the World Health Organization (WHO) on best practices in the pharmacy. Six components of the mission of the pharmacy profession were defined: being readily available to patients with or without an appointment, identifying, managing and detecting health problems; promoting health care; ensuring the effectiveness of medicines; preventing harm caused by them, and making a responsible use of limited health care resources. In this context, pharmacists made significant improvements in both the dispensing and administration of vaccines in the last decade.
In Latin America, pharmacists are often the first health care professionals that people consult, as visiting a physician is not as easy, affordable or fast as visiting a pharmacy.
Prevention is among the roles that pharmacists can perform as members of the health care system, one of which lies in promoting immunization in the population. It is essential to dispense and administer vaccines properly, as well as educate and raise awareness about vaccines for the prevention of infectious diseases. Marcelo Peretta and Carina Cremona, prestigious Argentine pharmacist advocators of the role of pharmacists, highlight the impact of these health care professionals in public health: «Pharmacists can expand their services and improve public health if they choose to work on vaccine preventable diseases of high risk groups”13.There is a lack of understanding about the role of the pharmacists and pharmacies in delivering vaccinations to the general public in Latin America. Such understanding would underscore the importance of pharmacists to address vaccination gaps in the region. The purpose of the study is to understand the policies and practices on pharmacy delivered vaccination in six countries of the region: Argentina, Brazil, Chile, Colombia, Mexico, Venezuela. The results provide essential information useful in decision-making and implementation of policies that can significantly impact public health in Latin American countries.
MATERIAL AND METHODS
Study design
A descriptive survey study was designed especially for this study to understand the policies and practices around pharmacy-delivered vaccinations in six Latin American countries: Argentina, Brazil, Chile, Colombia, Mexico and Venezuela.
Target population
The survey target populations were vaccination experts of pharmacies, pharmacy professional organizations, and universities with expertise in understanding the policies and practices of immunizations of the selected Latin American countries.
To identify knowledgeable experts, a database was elaborated based on registries obtained from national pharmacy confederations, scientific societies, academies or councils, universities and public health institutions from each country. In addition, information was gathered from international organizations such as FIP, WHO, and the Pan-American Health Organization (PAHO).
Two to six experts from each country were selected by convenience sampling according to the inclusion criteria listed below.
Inclusion criteria
To participate, experts had to be an opinion leader/representative of at least one of the Latin American countries of interest (Argentina, Brazil, Chile, Colombia, Mexico or Venezuela), they must have a health-related degree (pharmacist, physician, nurse) with a pharmaceutical practice/public health orientation and/or considered an expert on policies and practices of pharmacy-delivered vaccinations.
The expert considered to be representative of a selected Latin American country was required to be currently living in that country.
Participants must meet at least one of the following criteria:
• Opinion leaders/benchmark of a national pharmacy chain.
• Active member of a national pharmacist professional organization; representative of a national pharmacy institution such as federations, confederations, societies, academies, universities, councils.
• Person who has worked or is currently working as a faculty member, or who has at least fifteen years of expertise in the field of pharmaceutical practice focused in primary health care.
• Person who has collaborated or is collaborating with the government in developing policies on public health and/or in training pharmacists.
• Person who is actively engage with public health affairs regarding pharmaceutical practices; researcher on the field (role of pharmacists in primary health care).
Experts were contacted via email and phone calls and communicated the study objectives. After the study objectives were communicated to them, an agreement on the activities and on the extent of involvement of each participating opinion leader in the study had been reached.
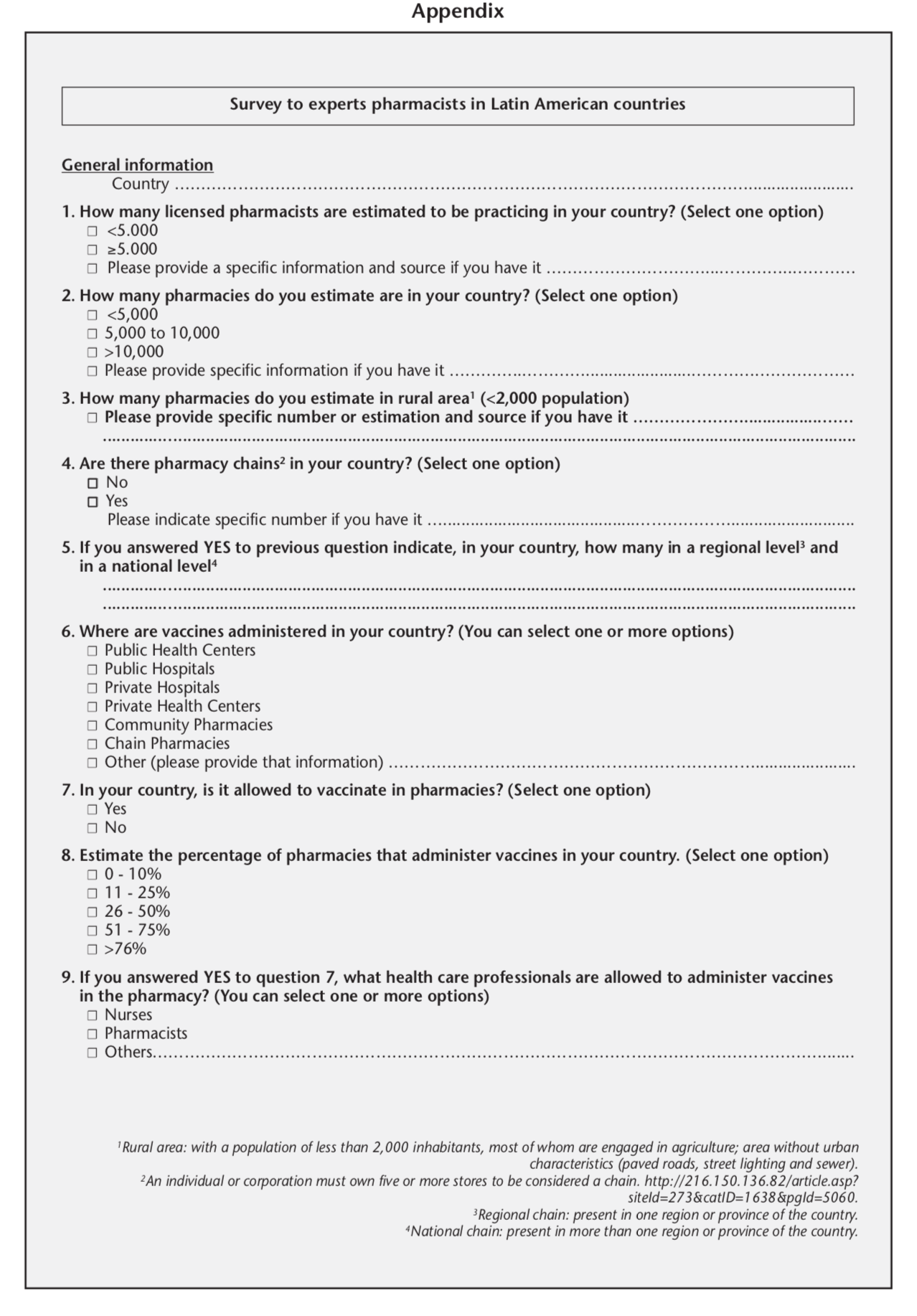
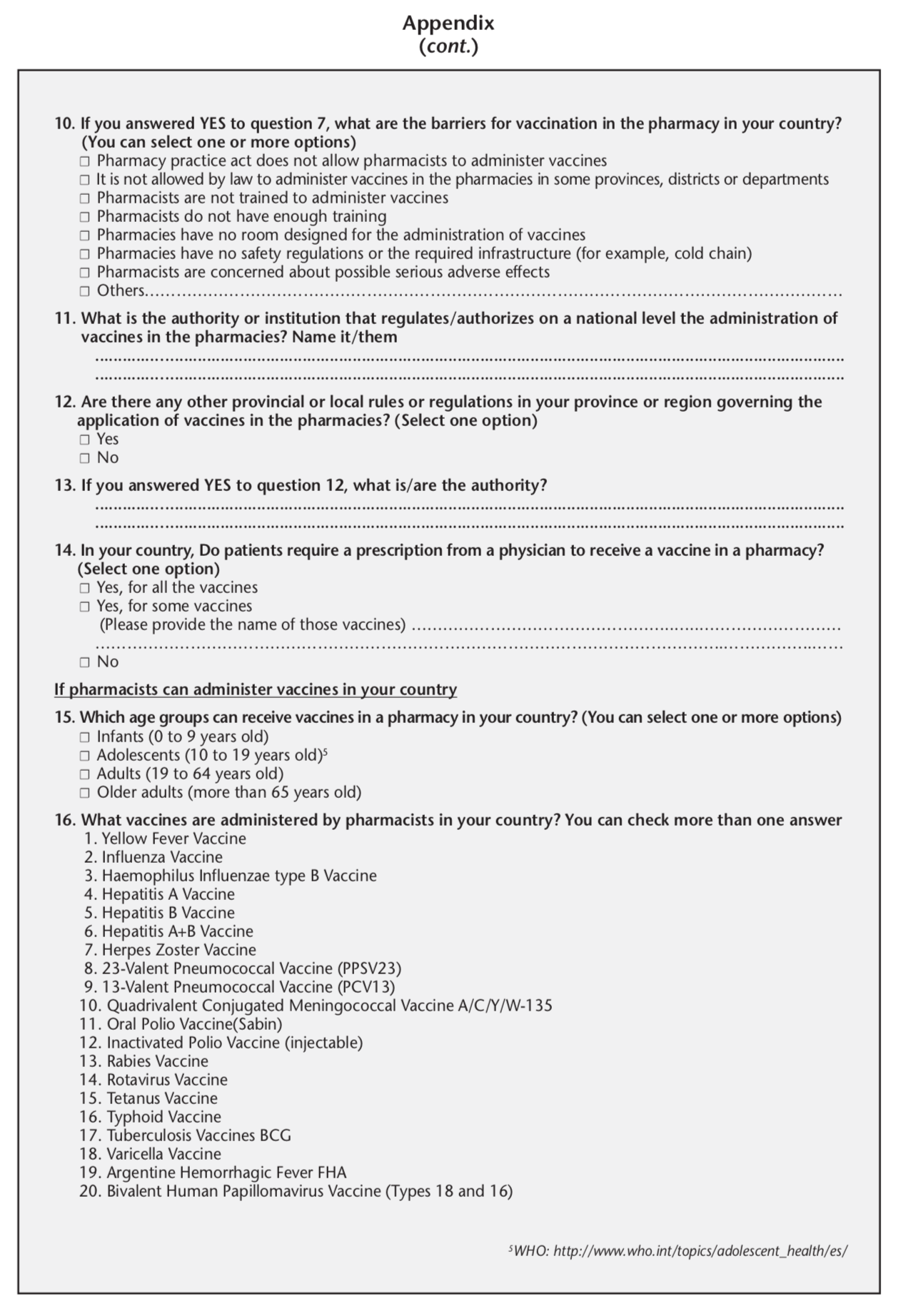
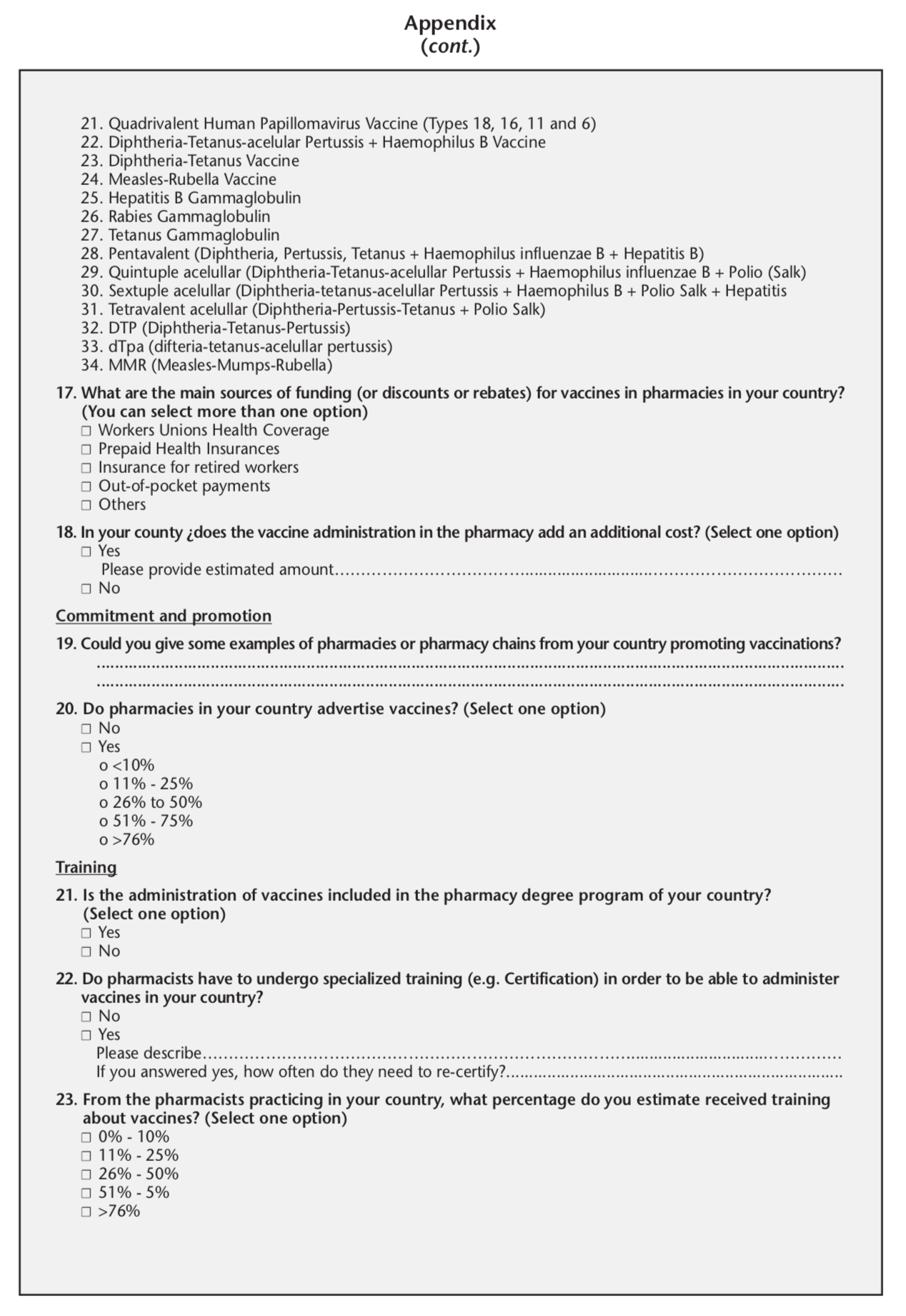
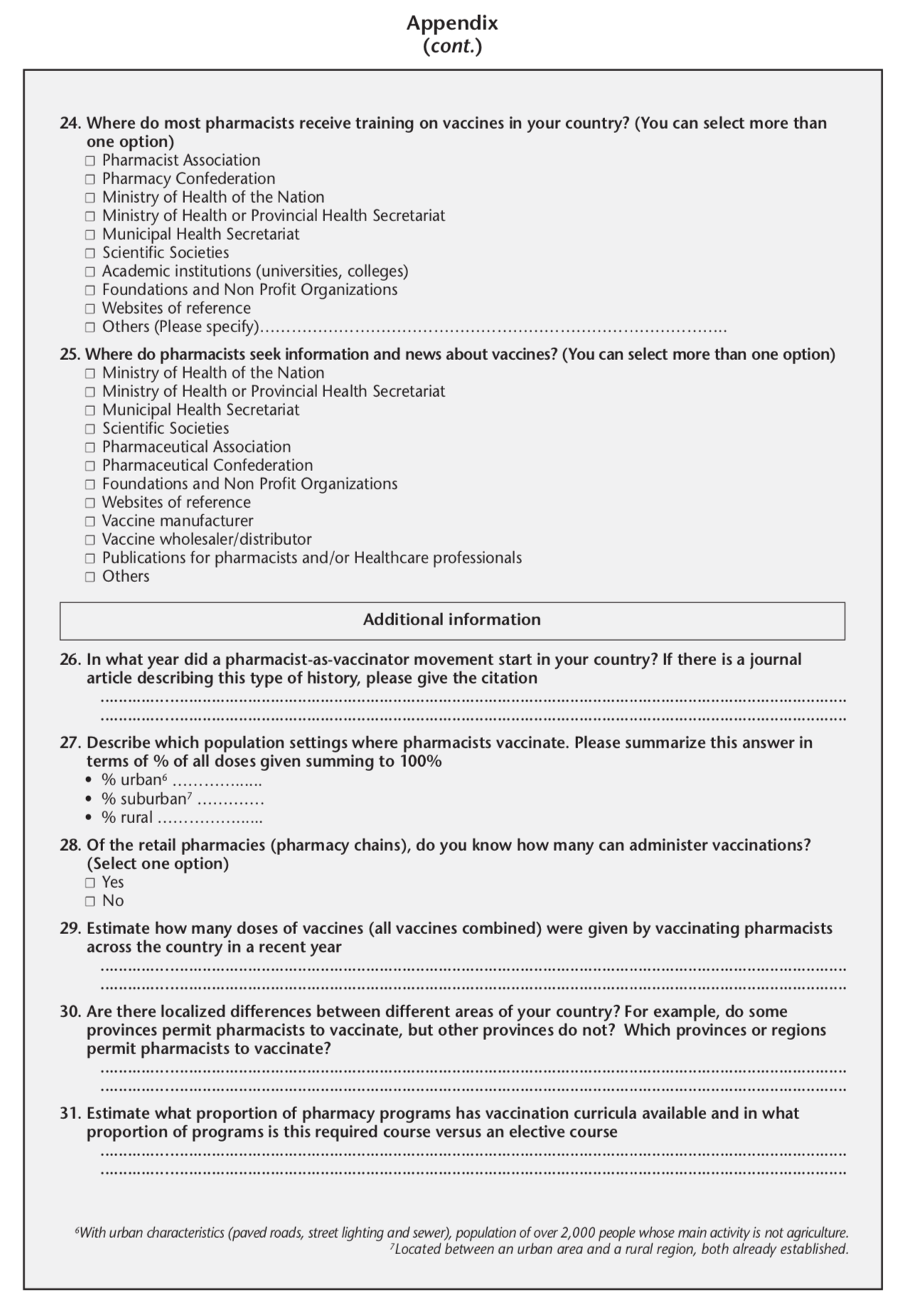
Survey design and measures
A specific survey (Appendix) was designed ad hoc to explore and describe information regarding topics such as common vaccination practices in pharmacies in the region, barriers for vaccination in pharmacies, underlying policies as well as prescriptions requirements for vaccines, and reimbursement policies.
The selected experts were contacted during a three month period. A link was sent to their email address in order to have access to an online survey. The survey ran on an open source framework available through the internet and accessible from any device (PC, cell phone, tablet, etc). The respondents had one month to complete the survey since they first access to it. They were able to enter as many times as needed within that month. If a question took them more time to be responded they had the chance to save the information already entered and answer it at a later time.
The survey was divided in five domains and leaders had the possibility to navigate through them and answer questions at different times if needed.
All responses were anonymous. Contacts received telephone calls and email reminders once a week.
The survey comprised five dimensions: general information, policies and regulations for vaccine administration, vaccine administration and promotion, training, and additional information. All the domains were mandatory to answer except the one of additional information.
Dimension 1: General information
– Licensed pharmacists: Number of authorized pharmacists that are allowed to work in pharmacies.
– Total pharmacies: Total number of pharmacies existing in the country under study.
– Total rural pharmacies: Total number of rural pharmacies in the country under study.
– Existence of pharmacy chains: The existence or not of pharmacy chains in the country under study.
– Number of pharmacy chains at national and regional levels: The total number of pharmacy chains at a local, provincial, state, county level and the total number of pharmacy chains in the country.
Dimension 2: Policies and regulations for vaccine administration
– Place of vaccine administration: Public or private places in the country under study where the administration of vaccines is authorized.
– Vaccination in pharmacies: whether vaccination is permitted or not in pharmacies, according to the national vaccination regulations.
– Percentage of pharmacies that administer vaccines: Percentage of pharmacies that are allowed to administer vaccines and do that practice.
– Vaccine administration in pharmacies: Health care professional/s that is/are authorized to administer vaccines in pharmacies.
– Barriers for vaccination in pharmacies: Circumstances perceived by the pharmacist or regulations that prevent or hinder the application of vaccines in pharmacies.
– Authority that regulates the administration of vaccines in pharmacies: Name of the national authority or institution that is in charge of regulating vaccines administration in pharmacies.
– Local rules or regulations: Whether provincial or local regulations or policies govern the application of vaccines in the pharmacies in addition to the national ones.
– Prescription for vaccination: Whether a prescription from a physician is required or not when receiving a given vaccine.
Dimension 3: Vaccine administration and promotion
– Population vaccinated in pharmacies: Age groups that are allowed to receive vaccines in a pharmacy.
– Vaccines administered by pharmacists: Vaccines that are legally permitted to be administered by pharmacists in pharmacies.
– Sources of funding: The main sources used to pay vaccines in pharmacies.
– Vaccination additional cost: The existence of an extra cost when people are vaccinated in pharmacies.
– Pharmacy promotion: The percentage of pharmacies involved in encouraging vaccination.
Dimension 4: Training
– Vaccine-related contents in Pharmacy degree program: The existence of specific vaccine administration modules in Pharmacy degree programs.
– Training on vaccines: Percentages of pharmacists who are currently practicing and receive training about vaccines.
– Place where training on vaccines is received: Place where pharmacists receive training about vaccines.
– Place where pharmacists seek information about vaccines: Place where pharmacists look for information regarding vaccines.
Dimension 5: Additional information
– Pharmacist-vaccinator movement: Whether or not the country under study had/has a pharmacist as a vaccinator movement.
– Population settings where pharmacists vaccinate: Proportion of all doses given according to the setting where pharmacist vaccinate (% urban, % suburban , % rural).
– Vaccination in retail pharmacies: Number of pharmacy chains that administrate vaccines.
– Total number of vaccine doses given in a recent year: Number of estimated doses of vaccines (all vaccines combined) given by vaccinating pharmacists across the country in a recent year.
– Law or regulation differences among provinces: Localized differences regarding vaccination regulations between different areas of the country under study.
– Pharmacy programs: Proportion that have vaccination curricula available and in what proportion of programs this was a required course versus an elective course.
Data collection and analysis
Data was collected online and reported as frequency measurements expressed in percentages.
To ensure confidentiality of the information, an exclusive server was designed for the project, and the principal investigator and project managers used a personal access code (username) and password.
The online database, which was specifically designed for the study, ran on an Open Source framework available through the Internet, accessible from any device (PC, tablet, cell phone, etc.) that supports Mozilla or Chrome browsers. The administration panel was accessible only by the administrator’s username and password. As the survey was anonymous the project manager, research team and data analyst could not modify the data. It could only be changed from the coordinating center.
The data was exported from the platform into MS Excel (Microsoft Corporation, Redmond, WA, USA), which allowed the analyses of the information gathered.
The results of the survey were uploaded to a database ad hoc through two data entries and both of them were cross-referenced to consolidate the information.
RESULTS
Twenty-three experts from the six Latin-American countries completed the survey. We reached a response rate of 74%. In four of the six countries, respondents indicated that pharmacy-based vaccination is allowed. There were discrepancies noted among the respondents surveyed in Brazil, Chile and Colombia (Figure 1).
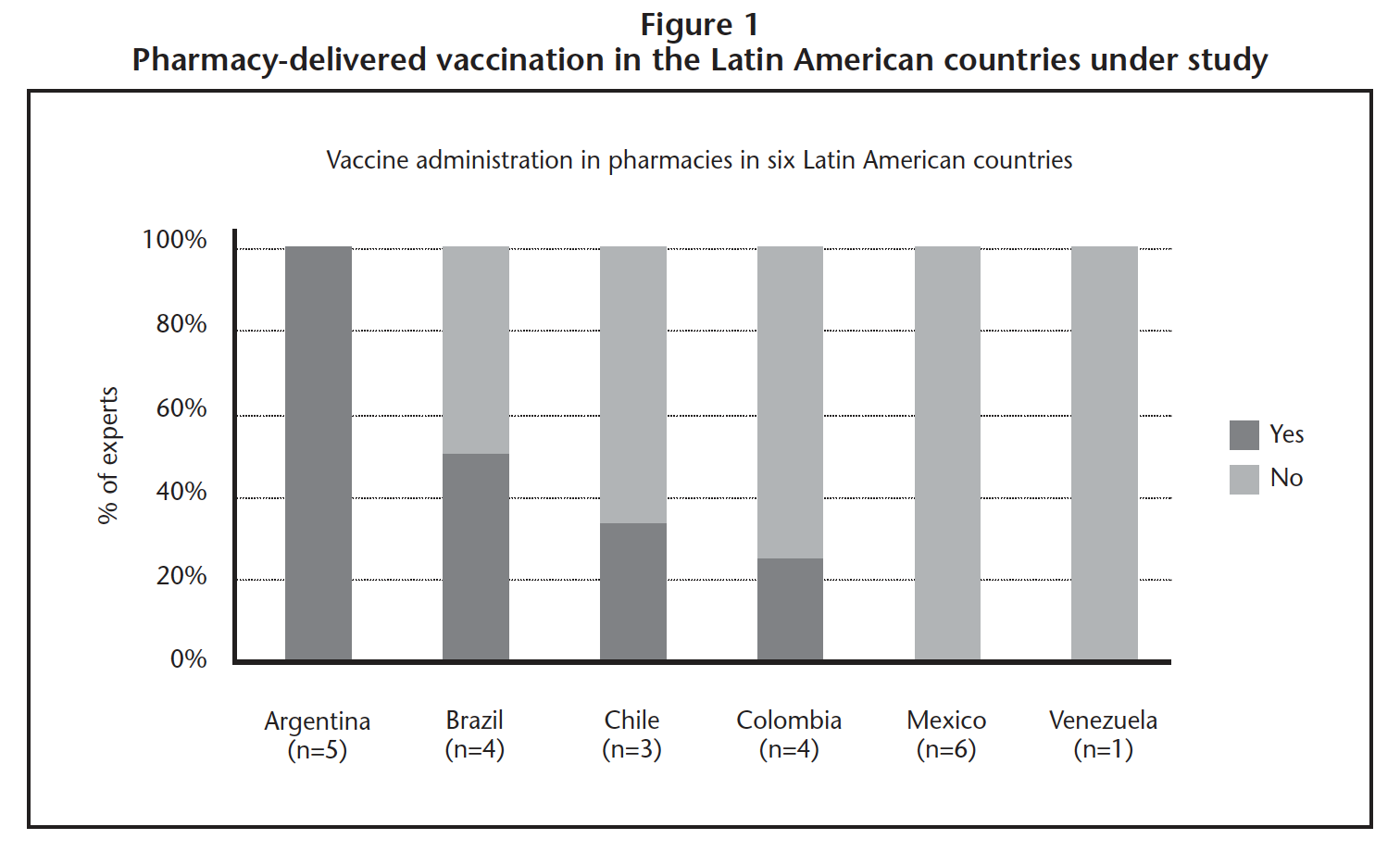
In Argentina, respondents stated that around 65% of pharmacies administer vaccines. In the countries where answers were divided, experts responded that less than 10% of pharmacies immunize. Among those who answered for Argentina, Brazil and Colombia that vaccines are given in pharmacies, 100% of their responses included pharmacists and nurses as responsible for vaccination, while in Chile only paramedics were mentioned.
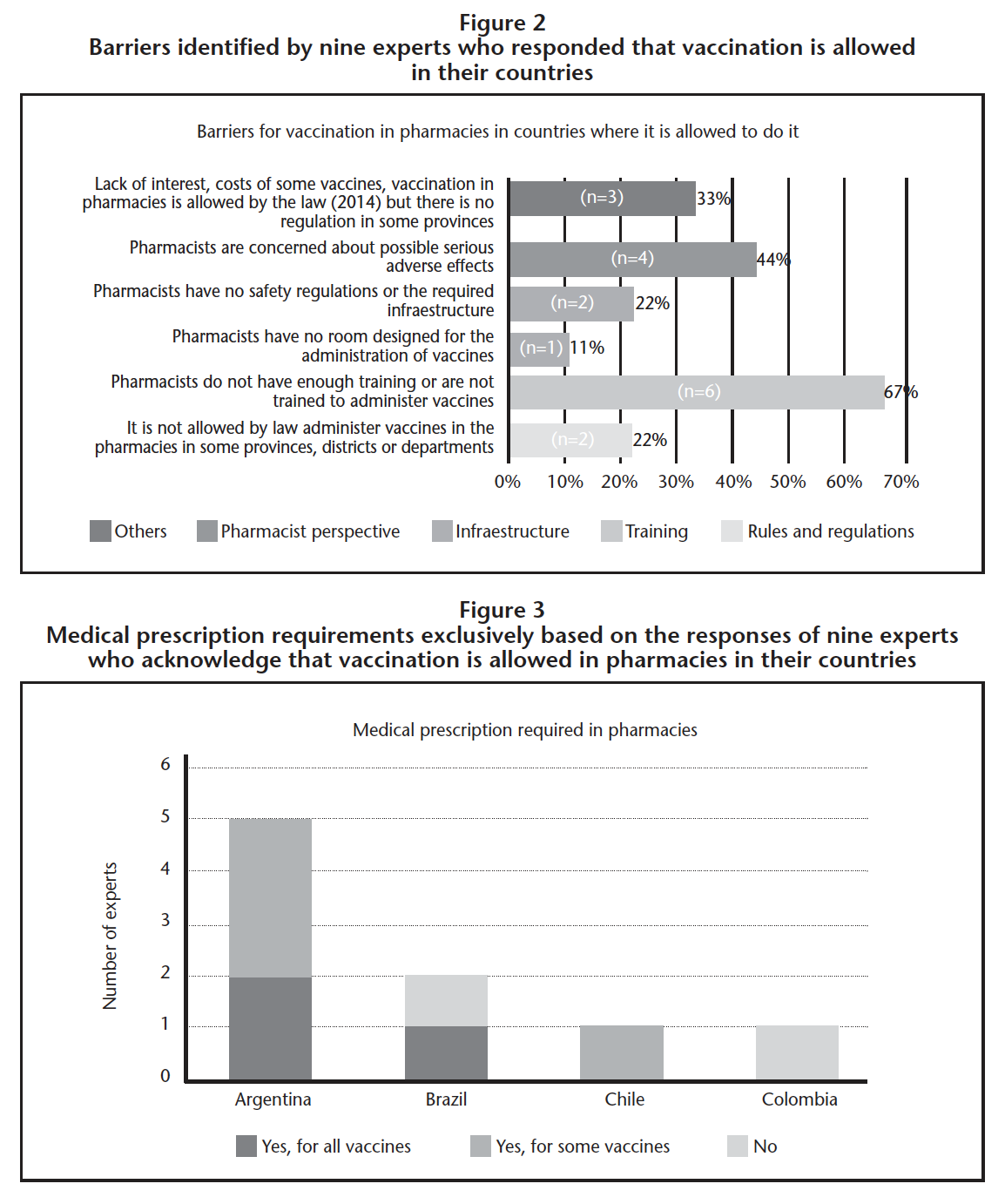
Barriers for pharmacy-delivered vaccination include: lack of enabling rules and regulations (22%), pharmacists’ perspective (44%), training (67%), infrastructure (33%) and others (33%) (Figure 2).
Need of a medical prescription (MP) to receive a vaccine in the pharmacy varies by country and by respondent (Figure 3).
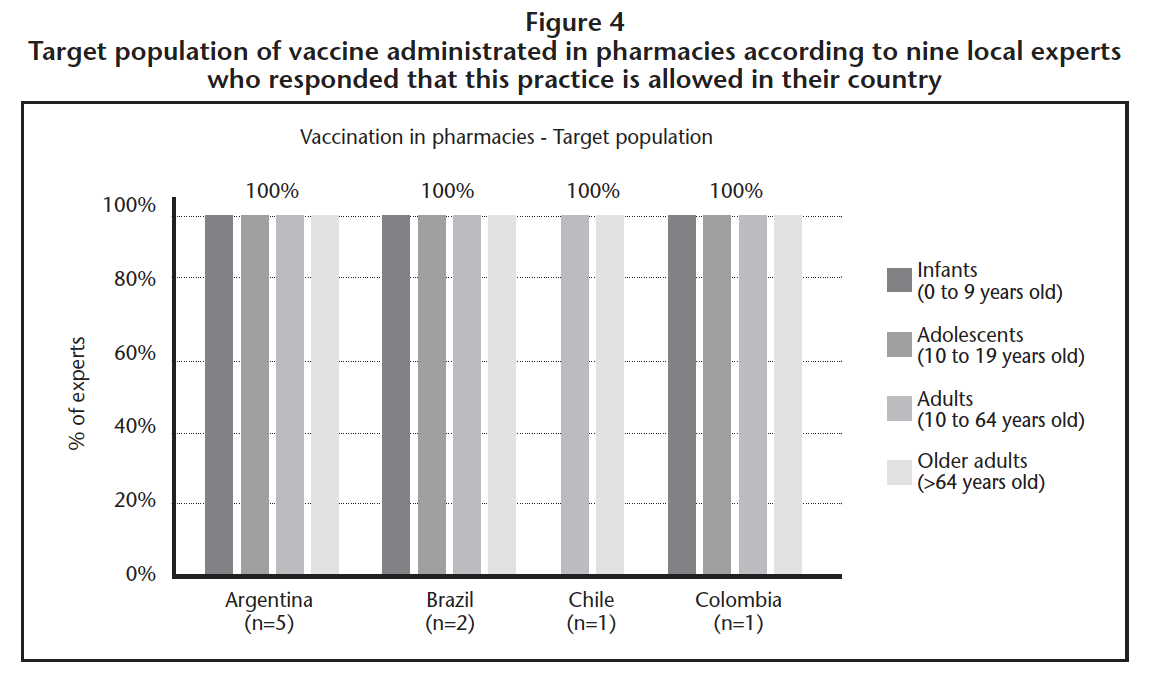
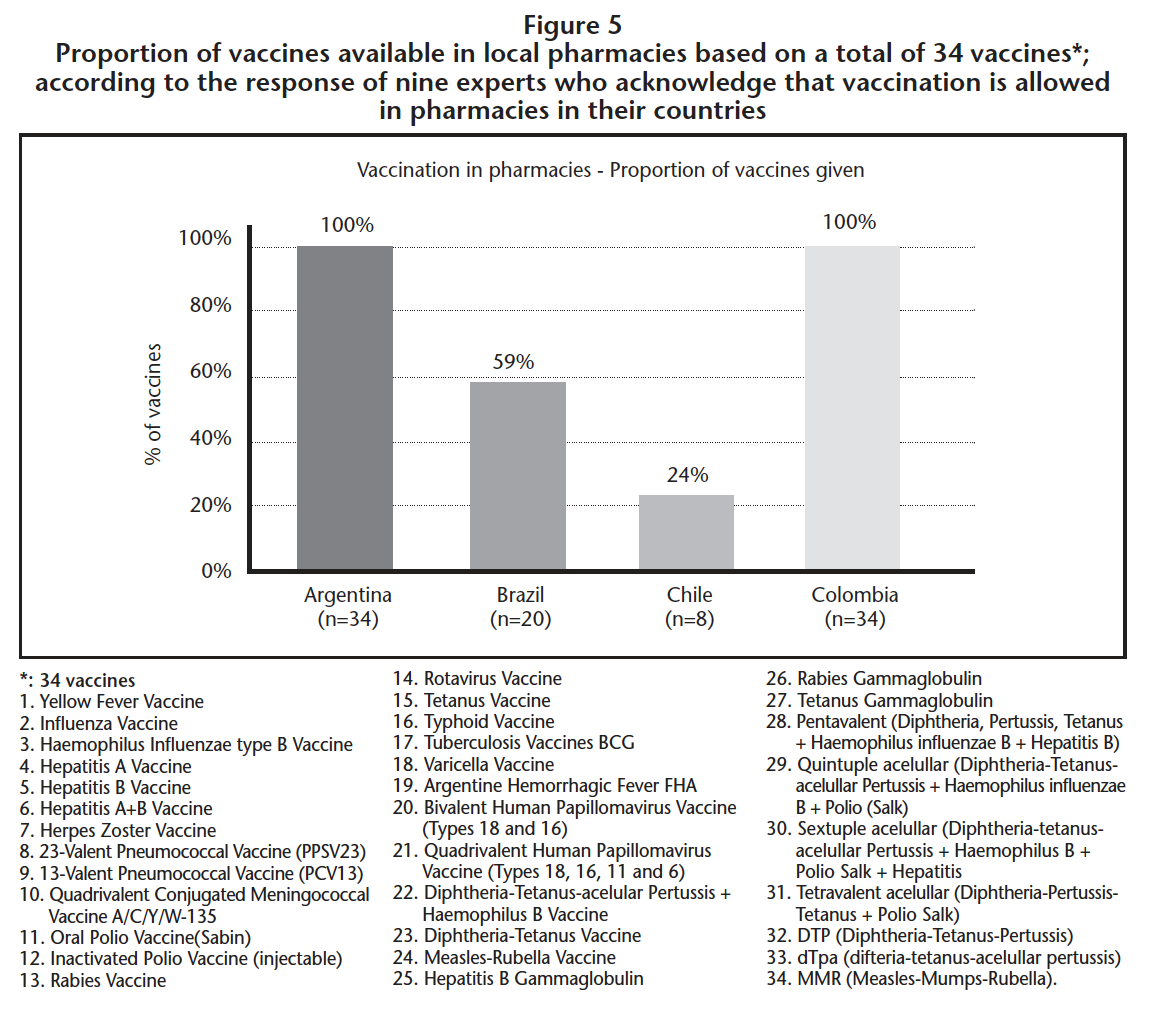
In Argentina all available vaccines are offered in pharmacies and to all age groups. In countries where the answers regarding rule or regulation to vaccinate in pharmacies are divided, not all vaccines are offered nor are all age groups included (Figures 4 and 5).
DISCUSSION
Results of this descriptive study show that policies and practices around pharmacy-delivered vaccination are diverse in the six Latin American countries and within each country under study, which is consistent with previous research14,15.
Argentina and Mexico are two opposing examples where experts were consistent with their answers. In the first one, all experts agreed that vaccination is allowed in pharmacies while in the second one, all the respondents answered it is not. In Brazil, Chile, and Colombia, inconsistencies were noted among the respondents surveyed. Regarding Venezuela, the only participating expert stated immunization in pharmacies is not allowed, although the respondent indicated pharmacies as one of the places where vaccines are administered. We believe these discrepancies among experts might be the expression of unclear laws and/or regulations although it is inappropriate to come to a conclusion with the current study design.
In relation to the proportion of pharmacies that offer immunizations, in Argentina, respondents stated that around 65% of pharmacies engage in this practice while in the countries where answers were divided, experts responded that less than 10% of pharmacies immunize. This suggests that policies and regulations are not the only barriers encountered by pharmacists to vaccinate in pharmacies because in Argentina regulations seem to be clear when compared to Brasil, Chile and Colombia. According to the experts, in Chile vaccines are administered by paramedics. We found this interesting as in the rest of the countries pharmacists and nurses are the ones who have the role of vaccinators. Similarly to other studies, the most frequent barriers found for pharmacy-delivered vaccination include the lack of training on vaccination and pharmacist concerns about possible serious adverse events. Also, the difference in local rules and regulations in some countries is an obstacle to the adequate vaccine administration in pharmacies. However, pharmacists’ lack of vaccine knowledge and education, regulations, immunization liability and infrastructure were the most seen in different studies15,16.
When exploring the need of a MP to receive a vaccine in the pharmacy, the answers varied by country and by respondents. The two experts from Chile and Colombia, who answered that vaccination is allowed in pharmacies, responded that MP are required for some vaccines and that MP are not needed, respectively. On the other hand, in Argentina and Brazil answers were divided: all vaccines require MP, some vaccines need them and MP are not required. Discrepancies might emerge due to the coverage of vaccines by the National Immunization Program as well as by national campaigns, where most of the times a MP is not needed. An example for adult vaccine given by the experts that does not require MP when being part of national campaigns is the influenza vaccine.
When referring to the types of vaccines offered and the target immunized population in pharmacies, in Argentina and Colombia all available vaccines are offered and to all age groups. In Brasil vaccines are administrated to all age groups but not all vaccines. And in Chile not all age groups are included nor are all vaccines are offered.
Having a better understanding of regional and local policies and regulations is useful to identify possible roles for pharmacist, such as those proposed by Grabenstein and colleagues17, (pharmacist as vaccine advocate, as facilitator and as immunizer), to improve vaccine promotion and disease prevention. According to our study results, pharmacy commitment and promotion about vaccines is very low in five of the six countries under study (except Argentina). There is evidence showing that pharmacy vaccination advertising and promotion facilitates pharmacy customers to get vaccinated18,19.
Isenor and colleagues published a systematic review and meta-analysis5 assessing the impact of pharmacists in vaccination activities. An increased in immunizations was shown, regardless of the pharmacist’s role (vaccine advocate, facilitator or administrator). Although the study included non-randomized trials and there was heterogeneity among them, it suggests that pharmacists are a key piece of the puzzle to improve immunization rates. Moreover, there is promising evidence showing that immunization training as part of pharmacy curricular requirements and as certified programs to improve vaccination among specific adult populations20.
Although in some countries laws and regulations might be clear, lack of knowledge among health professionals regarding the policies and practices of pharmacy-based vaccinations are still present which may be hindering adult immunization. The impact of including immunization training in pharmacy degree programs should be adequately assessed as well as understanding public and pharmacists’ perceptions regarding acceptance of pharmacists as immunizers. Future research is needed to explore national initiatives and strategies to be implemented to overcome patient’s and pharmacist’s access barriers to immunization to finally increase adult vaccination rates in the region.
LIMITATIONS
Limitations of this study include the small sample size which may not necessarily be representative of the Latin America region. The availability, reliability, and accessibility of respondents’ data may also vary by country. However, respondents selected by convenience sample have a health-related degree (pharmacist, physician, nurse) with a pharmaceutical practice/public health orientation and/or considered an expert on the policies and practices of pharmacy-delivered vaccinations. The inclusion of medical doctors, who are the main health professional committed to vaccinations and who patients more listen to, is one of the strengths of the study. Despite the surveys were anonymous and we were unable to identify the experts to clarify discrepancies, still many of them provided the citation of the information given.
CONCLUSIONS
Policies and practices around pharmacy-delivered vaccination in the Latin American countries under study are diverse based on the experts’ responses. In Argentina and Mexico there is a clear law that regulates vaccination in pharmacies. In contrast, in Brasil, Chile and Colombia, the variability in responses highlights the existence of ambiguous understanding of the laws and regulations. In Venezuela, information was scarce due to the lack of the minimum number of participants. It is evident that pharmacies do not vaccinate in all Latin American countries. Increased efforts should be taken to fully understand policies around vaccination in Latin America and how policies can be implemented in countries where pharmacists do not vaccinate. Future work will be developed to overcome barriers and highlight the role of pharmacists as educators, facilitators and/or administrators of vaccines.
Conflict of interest: Authors state that this is a descriptive study and does not require a signed inform consent. The survey was anonymous and research did not represent a risk to the participants.
Source of funding: This study was funded by MERCK SHARP & DOHME CORP.
Bibliography
1. World Health Organization. Immunization coverage. Fact sheet. [Internet]. Updated July 2016. Disponible en: http://www.who.int/mediacentre/factsheets/fs378/en/.
2. Skelton JB, American Pharmacists Association & Academy of Managed Care Pharmacy. Pharmacist-provided immunization compensation and recognition: white paper summarizing APhA/AMCP stakeholder meeting. J Am Pharm Assoc. 2011;51(6):704-12.
3. American Pharmacists Association. American Pharmacists Association 2014 Annual Report Advancing as one [Internet]. Disponible en: http://media.pharmacist. com/APhA/2014_APhA_Annual_Report.pdf.
4. Grabenstein JD, Guess HA, Hartzema AG, Koch GG, Konrad TR. Effect of vaccination of community pharmacists among adult prescription recipients. Med Care. 2001;39(49):340-48.
5. Isenor J, Edwards N, Alia T, Slayter K, MacDougall M, McNeil S. Impact of pharmacists as immunizers on vaccination rates: a systematic review and meta-analysis. Vaccine. 2016;34:5708-23.
6. Harris KM, Uscher-Pines L, Mattke S, Kellermann AL. A Blueprint for Improving the Promotion and Delivery of Adult Vaccination in the United States. Santa Monica [Internet]. RAND Corporation: 2012. Disponible en: http://www.rand.org/content/dam/rand/pubs/technical_reports/2012/RAND_TR1169.pdf.
7. Grabenstein JD. Pharmacists as vaccine advocates: roles in community pharmacies, nursing homes, and hospitals. Vaccine. 1998;16:1705-10.
8. Grabenstein J, Stanley D. Beyond influenza: strategies for implementing other adult vaccines into practice. J Am Pharm Assoc. 2001;41(suppl 1):S32-3.
9. Hogue MD, Grabenstein JD, Foster SL, Rothholz MC. Pharmacist involvement with immunizations: a decade of professional advancement. J Am Pharm Assoc. 2003;46:168-79, quiz 179-82.
10. Fletcher A, Marra F, Kaczorowski J. Pharmacists as vaccination providers: Friend or foe? Can Pharm J (Ott). 2014;147(3):141-42.
11. Canadian Pharmacists Association. Expanding the Role of Pharmacists [Internet]. 2012. Disponible en: http:// www.pharmacists.ca/cpha-ca/assets/File/education-practiceresources/Translator2012V6-3EN.pdf.
12. World Health Organization. The role of the pharmacist in the Health Care System. Preparing the Future Pharmacist: Curricular Development. Report of the third WHO Consultative Group of the Role of the Pharmacist. 27-29 August 1997 [Internet]. Vancouver, Canada: WHO; 1997. Disponible en: http://apps.who.int/medicinedocs/pdf/h2995e/h2995e.pdf.
13. Peretta M. Reingeniería farmacéutica: principios y protocolos de atención al paciente. 2da edición. Buenos Aires: Editorial Médica Panamericana; 2005.
14, International Pharmaceutical Federation (FIP). An overview of current pharmacy impact on immunisation – A global report 2016 [Internet]. The Hague: International Pharmaceutical Federation; 2016. Disponible en: http:// fip.org/files/fip/publications/FIP_report_on_Immunisation.pdf.
15. Sauvageau C, Dubé E, Bradet R, Mondor M, Lavoie F, Moisan J. Immunization services offered in Québec (Canada) pharmacies. Hum Vaccin Immunother. 2013;9(9):1943-9.
16. Edwards N, Gorman Corsten E, Kiberd M, Bowles S, Isenor J, Slayter K, et al. Pharmacists as immunizers: a survey of community pharmacists’ willingness to administer adult immunizations. Int J Clin Pharm. 201; 37(2):292-5.
17. Grabenstein JD. Pharmacists as vaccine advocates: roles in community pharmacies, nursing homes, and hospitals. Vaccine. 1998;16(18):1705-10.
18. Grabenstein JD, Guess HA, Hartzema AG. People vaccinated by pharmacists: descriptive epidemiology. J Am Pharm Assoc. 2001;41(1):46-52.
19. Marra F, Kaczorowski J, Gastonguay L, Marra CA, Lynd LD, Kendall P. Pharmacy-based Immunization in Rural Communities Strategy (PhICS): A community cluster-randomized trial. Can Pharm J (Ott). 2014;147(1):33-44.
20. Hogue MD, Grabenstein JD, Foster SL, Rothholz MC. Pharmacist involvement with immunizations: a decade of professional advancement. J Am Pharm Assoc. 2003;46(2):168-79; quiz 179-82.
____
____
Descargar artículo en PDF: Policies and practices on pharmacy-delivered vaccination: a survey study conducted in six Latin American countries